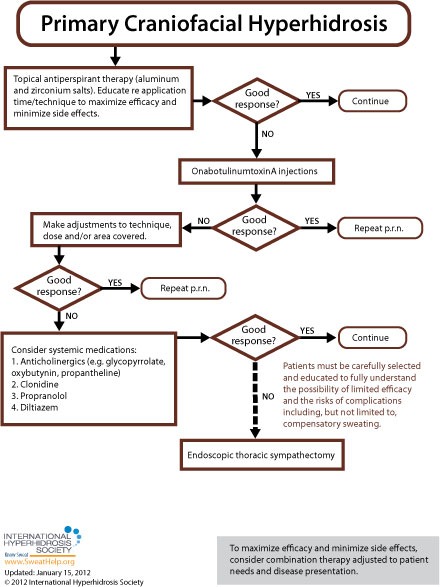
When approaching treatment to primary craniofacial hyperhidrosis as well as gustatory hyperhidrosis (Frey's syndrome) the general recommendation is to try more conservative therapy before resorting to invasive treatment. While each of the anatomic areas prone to excessive sweating is more or less susceptible to the various approaches available, [9] treatment guidelines for primary craniofacial hyperhidrosis and gustatory hyperhidrosis (Frey's syndrome) are as follows:
Gustatory Hyperhidrosis/Frey's Syndrome
For gustatory sweating, patients should initially be advised to avoid those foods that produce symptoms. Gustatory sweating (Frey's syndrome) can be controlled in part by avoiding foods known to stimulate sweating. Such foods commonly include coffee and other caffeinated products, chocolate, spicy or sour foods, hot foods, alcohol, foods or drinks containing citric acid, and/or sweets.[19,83,145] If avoidance of triggers provides the patient with insufficient relief, either topical antiperspirants or onabotulinumtoxinA injections are appropriate next steps.
A two-week trial of topical antiperspirants (with compliance to regimen) is usually sufficient to determine whether topical agents will work for a particular patient. [E] Topical antiperspirants can be very effective but are limited by irritation that is caused by the formation of hydrochloric acid in a chemical reaction between the aluminum chloride and sweat present on the skin surface. Application on a very dry, nonoccluded skin surface can reduce this irritation substantially. [A]
Generally, it's recommended that prescription antiperspirants containing aluminum chloride be applied before sleep (when sweating is at its most minimal) and washed off 6 to 8 hours later. [E] Skin should be completely sweat-free before product application [D] -- a cool blow drier or towel may be used, if necessary. Washing the skin before application is not necessary and may actually lead to greater irritation.
If skin irritation occurs, topical hydrocortisone cream treatment is often recommended. In the absence of skin irritation, the antiperspirant should be applied every night for 1 week until sweating is reduced. Once the antiperspirant has taken effect, the period between treatment re-application may be extended to once per week, or less frequently, as long as desired results are maintained. [B] Drawbacks of antiperspirants for any type of craniofacial sweating include a white sheen left on the face by the products and the potential for eye irritation. [G]
An equally acceptable first-line treatment for gustatory hyperhidrosis/Frey's syndrome is onabotulinumtoxinA. The U.S. Food & Drug Administration (FDA) has approved onabotulinumtoxinA for the treatment of severe primary axillary hyperhidrosis in patients unable to obtain relief with antiperspirants (July19, 2004). While only FDA-approved for axillary hyperhidrosis in adults, onabotulinumtoxinA can also be used for any area of focal hyperhidrosis and is commonly used in pediatric patients. [A] OnabotulinumtoxinA injections offer a minimally invasive treatment option and should be repeated as necessary to control symptoms. [99]
Generally patients receive 2 to 3 treatments per year for facial hyperhidrosis because the treatment effect has been reported to last a minimum, on average, of 5 months. Prior to treatment for craniofacial hyperhidrosis patients should be counseled about the potential for asymmetry of the brow. When brow asymmetry occurs it is usually transient lasting only a few weeks whereas the effect on sweat reduction lasts much longer. Minor muscle weakness that results in an inability to frown or furrow the forehead has also been reported.[G]
If the desired results are not achieved initially, practitioners are advised to make adjustments to technique, dose, and/or the area covered and repeat the treatment. Although some patients relapse shortly after their course of treatment, most studies report that a second set of injections will often provide effective symptom abatement. [C]
If the patient does not respond to or does not tolerate onabotulinumtoxinA, another therapeutic option to consider is the use of a systemic medication (glycopyrrolate, oxybutynin, propantheline, propranolol, clonidine, or diltiazem). Additionally, if symptoms are exacerbated in known anxiety-provoking situations, short-term expectant use of a benzodiazepine or anticholinergic may be considered. [9,19] International Hyperhidrosis Society experts have found that clonidine is especially useful for the treatment of facial hyperhidrosis and discussed this in a recent webinar. You can "watch the full video here."
Oral medications require patient education regarding potential side effects (such as dry mouth, blurred vision, urinary retention, tachycardia and constipation). These side effects may limit the use of anticholinergics in many patients [A, B] but sometimes can be managed by adjusting the individual's dose or by carrying a water bottle, using oral rinses, using eye drops, and/or adjusting diet for constipation. Before treatment with oral systemic medications for hyperhidrosis, extra consideration should be given regarding pediatric patients, people who participate in sports, people who work outdoors, and any other patients who may potentially cause themselves injury by becoming overheated. Physicians' notes to coaches and/or teachers for students in regards to sports and PE may be useful. Of interest to practitioners with pediatric patients, the FDA has approved (July 2010) a liquid form of the anticholinergic glycopyrrolate (brand name, Cuvposa) to reduce drooling in pediatric cerebral palsy patients – off-label use of this medication may provide flexibility when dosing for pediatric patients.
Many practitioners also find that combinations of therapies can be effective. For example antiperspirants to increase duration between onabotulinumtoxinA injections. Adapting and integrating different available options to meet individual patient's needs can improve satisfaction.
Primary Craniofacial Hyperhidrosis
Treatment for primary craniofacial hyperhidrosis is very similar to that of gustatory hyperhidrosis/Frey's syndrome with the difference being that topical antiperspirants historically recommended to be tried first and onabotulinumtoxinA second. A 2015 systemic review of medical literature, however, found that based on available evidence, topical glycopyrrolate, oral oxybutynin and intradermal botulinum toxin A may be recommended as first-line therapies due to their efficacy and safety.
In a British Journal of Dermatology study (2000), researchers found botulinum toxin A to be an effective and safe treatment for frontal hyperhidrosis, with the amount of sweat being significantly reduced 4 weeks after treatment. The effect lasted at least 5 months in nine of the 10 patients. All patients subjectively judged the treatment as very effective. Similarly, in another 2000 study (J Neurol.): "The effect of botulinum toxin A (BTX) was studied on 12 patients with idiopathic craniofacial hyperhidrosis... After 1-7 days the craniofacial sweating in the area injected had completely ceased in 11 patients and was mildly reduced in the remaining one... Although sweating has not yet recurred in most patients at follow-up periods up to 27 months, one patient had a relapse 9 months after treatment. "
Recommendations listed above regarding topical products and onabotulinumtoxinA apply with the additional option, more recently, of topical 2% glycopyrrolate. In 2022, researchers found in comparing topical 2% glycopyrrolate and intradermal botulinum toxin A injection for facial hyperhidrosis treatment that both modalities showed complete response in 75% of cases with a longer duration of action in botulinum toxin group up to 6 months. Side effects were minor and temporary. Both Hyperhidrosis Disease Severity Scale and DLQI showed statistically significant improvement after treatment. They concluded that topical glycopyrrolate 2% showed comparable results to botulinum toxin A in facial hyperhidrosis treatment with faster onset, but shorter duration of action.
Systemic medications are generally recommended as a third-line treatment for primary craniofacial sweating, after adjustments to regimen, technique, etc. with antiperspirants and onabotulinumtoxinA have been tried. Another difference between treatment guidelines for gustatory sweating and primary craniofacial sweating is that ETS may be attempted as treatment for primary craniofacial sweating. It is, however, a treatment of last resort. The evidence that ETS is effective for this indication comes from a small series of patients and the surgery is not as effective for facial/cranial sweating as for palmar sweating. [6,112] The most frequent and important complication is compensatory hyperhidrosis. Especially in patients who have undergone resection of the second thoracic ganglion, the risk of severe compensatory hyperhidrosis is higher, which may cause dissatisfaction with the procedure. [F]
 Download
Download

 Hyperhidrosis
Hyperhidrosis